Ticks and Travel –
A Deadly Peril
By
Lucy Leaf
|
|
Ticks and Travel – A Deadly Peril By Lucy Leaf |
Three Long Riders set out on separate journeys. Two returned home within two weeks. The third was near the end of her journey, returning home in a terrible state.
They weren’t historic journeys. This all happened in today’s world, within the past three years.
It wasn’t an accident or injury that caused them grief. It wasn’t the reality of life on the trail that was unexpected. It wasn’t continuous rain, a lightning strike, extreme heat, or an unexpected blizzard that brought the trip to an end.
It was the bite of a tiny insect.
And it was nothing any of them considered as a peril to their journey.
I was one of them, off on a long walking journey starting from my home in Maine. I expected to be gone a year, two, or three, a replica of a horse journey I had made in the U.S. forty years ago, only simpler. Before leaving, I had been bitten by a tick.
The others were horse travelers who had also incurred a tick bite. They were on the trail.
All of us found and removed an imbedded tick. We all experienced severe local
reactions including redness and pain at the site. Debilitating muscle and joint
pain followed. It was the profound fatigue, however, that stopped us in our
tracks. Early in my journey, I was walking 12-15 miles a day with a loaded back
pack. At home two weeks later, I could not walk a hundred feet without plopping
down on the ground to rest, and I could barely lift my 25 pound pack.
|
In 1973 Lucy Leaf set off on a 7,000 mile journey aboard a non-pedigreed horse named Igor. The duo travelled a northern route across the country from Maine to Oregon and then returned from California to Virginia via a southern route. Despite having led a very vigorous outdoor life, in 2011 a tick bite devastated Lucy’s health. Unmanageable pain spread from the tick bite across her body. The constant agony destroyed her appetite, kept her awake for days and eventually caused her to black out. She warned other Long Riders, “Having enjoyed good health all my life (and taken it for granted, no doubt) I'm amazed how quickly my health, which seemed prime only weeks ago, has gone completely south.” |
|
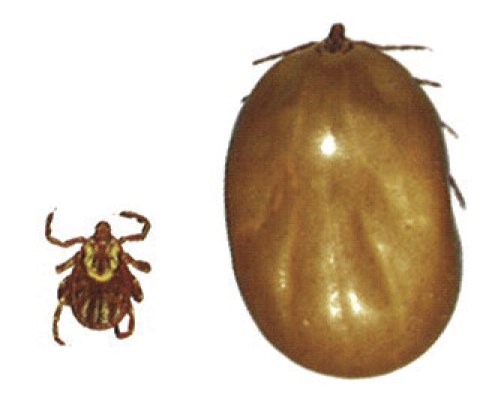
“Ticks are nature’s sewer”, a naturopath told me, “perfect reservoirs of disease.” Tiny as a pin head in their nymph stage, they wait patiently on the end of a twig or a blade of grass for a host to walk by. Their bite does not inflict pain, so they go unnoticed as they dig in and begin sucking the blood meal they need, slowly swelling to such a size that they finally drop off or get noticed by their human host. In the meantime, the pathogens lurking in their gut are conveniently injected into the bloodstream of the new host, where their life cycle continues. Not all ticks are infected with disease producing organisms, but any single specimen can be a vector for one or more of sixty conditions identified in the U.S. alone and many more worldwide.
Lyme disease is the one that has received the most attention. Since it became
reportable in the U.S. in 1991, it had increased threefold by 2009 to 38,000
cases, far exceeding HIV and West Nile Virus though the latter received a lot
more funding for research and prevention.
|
With the exception of mosquitoes, ticks pose the greatest danger to humans and horses, as they transmit a number of fatal diseases. Though only measuring 1 mm (3/64ths of an inch), ticks are ruthlessly successful predators that are capable of selecting ambush sites based upon their ability to distinguish well-travelled trails. Thanks to special sensory organs which allow them to detect the carbon dioxide emitted by horses and humans, they can sense the approach of their victims from a great distance. They take up a position on overhead branches or in tall grass and then wait for dinner to arrive. After they drop onto their unsuspecting host, they bury their head into the body and begin feeding on its blood. Their bites often go undetected because the tick injects an anaesthetic to deaden the injury. Thus, many victims remain unaware that they have been bitten. Once they are attached, a tick will feed for up to a week. At first it may resemble a small beige-coloured pea. Eventually the tick will become so bloated with blood that it resembles a child’s swollen thumb. Long Rider Ria Bosman reported that, during her journey through Africa, “Ticks swarmed over everything like black rain. At night when we got to bed, we had to examine each other by torch light and pull off ticks. Sometimes we removed as many as fifty from each other.” |
|
Living in the endemic Northeast of the U.S. where Lyme was identified in 1975, I
personally know well over a dozen people who have Lyme disease. That means they
have tested positive for Lyme, have debilitating symptoms, and are undergoing
treatment which can last for months, even years. Careers have been altered,
dreams have been crushed, lives have been reduced to day-to-day survival.
Families have gone deep into debt paying for prolonged and expensive treatment
not covered by health insurance.
Why?
Because the medical establishment in America refuses to recognize Lyme disease as a chronic condition.
People are bitten by a tick and their lives change.
“It’s not Lyme”, worried patients and parents hear time and time again from one doctor after another.
“So what is it then? What is it, Doc, that changed my son from an A- student and star athlete to a kid who can’t think or get out of bed, in just a matter of weeks?”
The diagnosis and treatment of Lyme disease is fraught in controversy and misinformation, directly affecting every person who sets foot on natural ground.
Consider the experiences of the three Long Riders, all of whom sought medical treatment following a tick bite. I myself was bitten by a wood tick, which is not the kind of tick known to spread Lyme disease. While a large circle of redness developed around the bite, it was not the classic “bulls-eye” rash that is associated with Lyme disease. So I waited three weeks before seeing a doctor who corroborated everything I had already read online from reliable sites such as the Center for Disease Control (CDC) and leading hospitals in the country.
The deer tick is the carrier of the Lyme disease. If it is not a deer tick, it
is not Lyme. The tick must be imbedded 24-36 hours before the bacteria are
injected from its gut. Even in an endemic area, with an observed tick bite there
is only a 1.2-1.4% chance of acquiring Lyme. And even if the tick is infected,
for most people, a two-three week course of antibiotics will eliminate the
infection. This is the information that both my doctor and I used to determine
that a ‘wait-and-see” approach was reasonable. Now I know that all this
information is highly misleading.
 |
Ticks transmit the bacteria which causes Lyme Disease. After being bitten, a distinctive mark MAY appear on the victim’s body. It resembles a large, circular red bull’s eye that is darker in the middle and lighter along the edges. But this mark does not always occur. Lyme Disease makes the victim miserable for weeks on end with flu-like symptoms and fatigue. Patients who go untreated have reported facial paralysis, arthritis, heart blockage, extreme fatigue, mental decline, irritability, depression, and other problems. |
I was told to monitor for any flu-like symptoms or neck or joint stiffness and I was given antibiotics for a skin infection which the doctor called “serious”. This antibiotic worked like magic and soon I was off on my long hike with hardly a thought about Lyme or any tick-borne disease.
Ten days later, I felt a strange pain emanating from the area of the tick bite, going down my leg and up my back. The pain was unresponsive to any pain medications I could buy over the counter. After three sleepless nights, I returned home for another visit to the doctor.
The doctor figured I had a back problem, though I assured him I had done nothing to hurt my back. Steroids and anti-inflammatories were prescribed and I was glad for the relief they provided. But the pain got worse, spreading across my entire torso. Now it took narcotics to get a few hours of sleep. Then numbness set in, though it also felt as though I were lying on a bed of needles. The physical therapist I saw said he never saw back pain that looked like my symptoms.
I lost all appetite. Food tasted strange. Attempting to climb a flight of
stairs, I passed out and crashed in a heap on the floor, square in front of
family members who carted me off to the hospital emergency room. The doctor
there recognized the possibility of Lyme and a test was ordered.
|
|
Many Long Riders are oblivious to the fact that ticks are more apt to ruin a journey than dangerous animals. There are, for example, “only” an estimated 70,000 wolves hunting in North America. Contrast the number of wolves against the estimated quintillion insects, 10,000,000,000,000,000,000, residing on the planet today. Don’t overlook the fact that there are 900,000 different types of insects and that 91,000 types reside in the United States alone. Thanks to these numbers, you can quickly realize the likelihood of you suffering from some type of negative insect-related experience while riding through the wilds. |
When results arrived positive for Lyme, I thought it was good news, believing that the standard three-week course of doxycycline, specific to the pathogen, would get me back on the trail again. Instead, I felt worse. I begged my doctors, of which there were several now, to extend the antibiotics to four, then five, then six weeks, which they did with great reluctance. I was treated as a narcotic seeker though I was desperate to get off them.
It seemed that none of the doctors I saw had any knowledge of Lyme disease except that the standard treatment should have eliminated it. I did improve enough to get off narcotics finally, but I was far from recovered. The doctors then referred me to an infectious disease specialist.
Attending a Lyme support group, I learned what I could expect as a “post-Lyme” patient. I would likely be re-diagnosed with chronic fatigue syndrome, fibromyalgia, and neurological disorders. Symptoms would be treated while the pathogens continued to spread.
Lyme can affect every system and organ in the body. I also learned what Lyme can lead to: debilitating arthritic pain, heart conditions, psychiatric disorders, and serious neurological disorders like multiple sclerosis and ALS or Lou Gehrig’s disease. Called “the great imitator”, Lyme disease mimics these conditions and is thought to also trigger them.
People die from Lyme disease. The spirochetes are relentless, settling into
parts of the body where antibodies are scarce and antibiotics harder to reach,
only to emerge again and wreak havoc later. But many patients do get relief
while on antibiotics, feeling a glimmer of hope for improvement and willing to
risk the side effects of prolonged antibiotic therapy.
| Swiss Long Rider Aimé Tschiffely faced many challenges during his epic journey from Buenos Aires to New York in 1925. While riding through Central America the ticks attacked his horses so savagely, Aimé devised blankets to help ward off the insects. |
 |
The support group strongly advised me to find a “Lyme-literate” doctor, though I would have to go out of state to find one. Waiting lists were long and insurance was unlikely to pay for it. Once the disease has disseminated, I was told, treatment involved weeks and months on antibiotics, which in chronic cases had to be administered intravenously. Doctors willing to treat chronic Lyme are at high risk of incurring malpractice suits or losing their license due to the public health concern over extended use of antibiotics. Patients with Lyme disease are a hot potato in a doctor’s office.
I thought my life was over.
I also learned that the steroids and anti-inflammatory medications I received for back pain likely worsened my condition, masking symptoms and compromising my immune system, allowing the infection to spread unchecked.
|
|
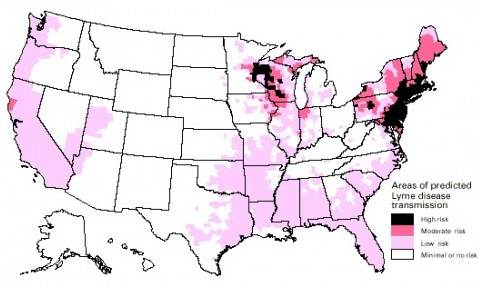
Warmer climates worldwide, and a general decrease in pesticide use, are helping encourage the proliferation of the tick population which in turn increases the number of cases of Lyme Disease. It is the most common tick-transmitted disease in the Northern Hemisphere. |
My salvation arrived in a brief email from a friend of a friend who had been successfully treated for Lyme by a naturopath. This young woman had been an outdoor educator, misdiagnosed by countless doctors and accused of malingering over a two- year period where she, too, could not climb a flight of stairs. The naturopath used modern Chinese medicine as the primary treatment modality, prescribing natural herbs that act as antibiotics along with herbs for immune support. He also used antibiotics, though sparingly. It was the treatment that had finally allowed his wife, a physician, to return to work after three years with Lyme where she could not add two and two, nor leave her home.
It would take six months of herbal treatment to be sure of a lasting effect, and though the alternative treatment cost me several thousand dollars, I have been symptom-free for the past two years, or at least, I think I have.
Another Long-Rider, BJ Stone, set out on horseback from her home in Texas this past summer, with plans to make a thousand mile ride around this very large state. Lyme is reported to be prevalent in areas of high atmospheric moisture, including the coastal regions of the U.S. and the Great Lakes. But this Long Rider set out into the dry Plains country.
|
The tick population has exploded in the United States, in part because of the dramatic expansion of the nation’s deer herds. In 1930 there were an estimated 300,000 deer in the country. Because of the decrease in hunting, and an aggressive campaign to protect deer from being culled, that number has now exploded to 30 million, with some areas complaining of 50 to 100 deer per square mile. Having lost their fear of man, the semi-tame deer venture out of forested areas lying close to human settlements. They boldly walk through neighbourhoods, feed in backyards and patrol state parks. That’s bad news for Long Riders because 95 percent of tick eggs come from ticks feeding on deer. One deer can feed 450,000 to 1,000,000 tick eggs per season. The more deer, the more ticks, and the higher risk of disease. |
Twelve days into the trip, BJ found a tick on the inside of her wrist and was able to remove it in its entirety, disinfecting the site carefully. Nevertheless, the site became very swollen and red, the actual bite cratered and oozing pus. Since Lyme isn’t prevalent in Texas, she wasn’t thinking about any complications beyond a superficial infection, though she had thought to protect her horse with a spray effective against ticks as well as other insects. But when red streaks ran up her arm, she decided to visit the hospital emergency room.
The first doctor didn’t know as much as she did about tick bites, ignoring the symptoms mentioned of extreme fatigue, stiff neck, nausea and aches. The second one she visited did no physical exam, but was willing to prescribe a course of doxycycline for two weeks only. When the Long Rider went to fill it, however, she found there was a shortage of this very common antibiotic.
The doctor was ready to switch to another antibiotic that would take care of the immediate infection only, but the concerned Long Rider persisted in getting what she needed. It was the pharmacist who helped her find it.
Once treatment began, she also felt worse before she felt better, but no medical professional warned her about this possibility, which I myself learned from the support group. During treatment, the die-off of bacteria can produce a toxic effect.
The infection on her wrist and arm cleared but several months later, she continues to have bouts of fatigue and body aches. Having to pay for further medical care or testing which can be unreliable, she has given up on medical doctors, preferring to work with a chiropractor/naturalist who takes her condition seriously.
In spite of all these challenges, BJ still plans to continue her ride in the spring.
Contrast this quality of care with that of a third very experienced Long Rider.
Mefo Phillips was bitten by a tick in June of 2010 while riding across the Massif Central in France on part of the Pilgrim Way to Santiago de Compestela. Traveling rough, she hadn’t washed her hair in ten days. When she finally had the opportunity to do so, “a very angry looking tick scrubbed out”, with a piece of her scalp in its jaws. Mefo figures it could have been there for a week. Near the end of her three-week journey, it was another week before she was able to get home to the UK and straight to an emergency facility. By then she had a high fever and headache, and had “ached liked fury” for four days.
The UK doctor didn’t know much about tick bites, but he took the time to investigate. His decision was to take no chances. This Long Rider was started immediately on a course of doxycycline. She then saw her own doctor who extended the course, though the tests came back negative for Lyme, not once but twice. Nevertheless, this Long Rider continued to be ‘knocked out” for a month or two, but has since recovered.
Researching her symptoms later, Mefo believes she may not have had Lyme disease, but another one of the diseases ticks can transmit, called ehrlichiosis. The high fever she experienced initially along with a purple rash that developed on her leg at a later date would be indicative of this bacterial infection which is also spread by a tick bite.
| Lucy Leaf was wounded by a tick in Maine. British Long Rider Mefo Phillips (right) was bitten during her summer-time journey across France and Spain. Yet the Long Riders shared one thing in common. Neither realized that, unlike a rattlesnake bite, it may take days or weeks for the tiny tick’s bite to take full effect. In both cases, it was too late for either Long Rider to ward off the infection which might have otherwise been prevented. |
|
A recent article in the New York Times proposes that chronic Lyme conditions may well be a manifestation of the concurrent infections which can result from the same tick bite. But testing for co-infections is often unreliable, as it is for Lyme disease. And that is another problem associated with Lyme and tick-borne disease.
Most of the tests available for Lyme measure antibody response to the infection versus the presence of the bacteria themselves. The latter requires a culture and Lyme bacteria grow too slowly for this kind of test to be practical. But the antibody response in the body takes 4-6 weeks to develop after a tick bite, so early testing is likely to produce false negatives. Therefore, in the early stages after a tick bite, when early treatment could be quite effective, diagnosis is dependent on a clinical evaluation of symptoms, which can vary from doctor to doctor.
While a distinctive bulls-eye rash is now considered a positive indicator for immediate antibiotic treatment, it is seen in less than half the patients who incur a tick bite and later test positive for Lyme. To complicate matters further, 50% of people who develop Lyme symptoms and eventually test positive for Lyme are not aware they ever had a tick bite.
Even after the 4-6 week period, testing can fail to pick up Lyme disease. There is a difference in quality of laboratories and how they report results. Specific knowledge is required for thorough interpretation. Doctors who are unknowledgeable may depend only on the standard ELISA screening test which can miss half of the true cases if not followed up by the Western Blot which confirms it. Even then, false negatives can occur and even false positives which, though rare, can invoke antibiotic treatment that may not be necessary.
Chronic cases are difficult to detect because the body is not producing antibodies all the time. Doctors look for confirmation to justify extensive antibiotic treatment, so patients with persistent symptoms are often desperate to get a positive test and will spend hundreds of dollars for more direct tests which find the bacteria through DNA evaluation or antigen detection tests. Multiple tests may be required to get a sample that has the bacteria. And then there are the likely co-infections. There is nothing simple about Lyme and tick-borne disease.
Lyme disease is not new to this world.
Genetic material from the Lyme bacterium was found in a 5300-year old mummy discovered recently in the Alps. The disease was named for the small village of Lyme, Connecticut where a young researcher correlated the bite of a tick with an abnormally high incidence of arthritis seen in children of that area. But symptoms following a tick bite had been described in northern Europe as early as the mid 1700’s. The ring-like rash was observed following the bite of a sheep tick in 1909 and neurological symptoms were recognized in the early 1920’s.
It wasn’t until 1982, however, that the specific causative agent was identified, a spiral-shaped bacterium given the name Borrelia burgdorfer. Lyme disease has now been found on every continent except Antarctica, as are ticks, though different species of ticks carry the pathogen in different areas. B. burgdorfer is widely distributed in the northern hemisphere especially, reported extensively in Europe, England, the former Soviet Union, China, Japan, SE Asia, and S. Africa. It has been reported in every state of the U.S.
In 1877 Historical Long Rider Frederick Burnaby described the tick-infested caravanserais he encountered during his ride across Turkey. During Frank Heath’s 11,000 mile journey across the USA in 1925, he was forced to ride through areas of the country that were “abound with ticks”. The Lyme syndrome of today has had many names in the past, notably “sheep-tick fever”, which Long Rider Messanie Wilkins encountered on her ride across the U.S. in the 1950’s. Ten years ago, I aborted a hiking trip in the dry Sand Hills of Nebraska due to heavy tick infestation where I found 20-30 ticks crawling on me at once.
Has Lyme disease actually increased in recent years, or have we just become more aware of it?
Even this is controversial. Recently the CDC revealed that 30,000 cases are reported each year by state health departments, but the number of people that are actually diagnosed with Lyme disease is around 300,000, a tenfold difference.
Dr. Allen Steers, the Yale rheumatologist who put a name to the Lyme syndrome, devoted his career to the study of Lyme. He quickly developed a vaccine to prevent it. Initially, Steers was a hero to Lyme sufferers who could now pin their debilitating condition to a single bacterium which could supposedly be eliminated with simple treatment and vaccinated against. Ironically he is now seen as a villain to the much expanded Lyme community.
Now a professor of medicine at Harvard and frequently quoted by the American Medical Association, the CDC, and the Infectious Diseases Society of America (IDSA), Dr. Steers leads the way in denying that the condition he discovered exists in a chronic form. Of course, insurance companies are glad to use Dr. Steers as an icon for minimal treatment. While he has been harangued and threatened by families of Lyme victims unable to receive treatment, there is some validity to his position. A recent article in the New Yorker magazine, titled “The Lyme Wars”, describes the dilemma that medical professionals face.
Because Lyme symptoms, either acute or chronic, are similar to so many other conditions, Lyme has become the “junk-drawer diagnosis” for almost every kind of malady. Many people are receiving antibiotic treatment with no actual evidence of past or present Lyme that the medical community recognizes. Overuse of antibiotics does present a very real public health issue.
But the individual diagnosed with ALS, which is considered fatal in 2-5 years,
would certainly want to rule out the possibility that it could be Lyme disease.
Dr. Dave Martz, an oncologist diagnosed with ALS had this same thought. In
continuous pain, he had regressed to a wheelchair, requiring full-care
assistance. He tested negative for Lyme on both the ELISA and Western Blot tests
at two different laboratories. But knowing that the spirochetes can evade
detection in the blood, he submitted a urine sample for DNA testing and sure
enough, evidence of the Lyme pathogen was found. It took two years on a cocktail
of antibiotics and other medications, but he was able to regain normal function
and has been pain-free for the last seven years. His testimony at a recent,
highly attended conference on Lyme disease brought a new wave of hope to
long-term sufferers.
| Frank Heath was the first Long Rider to record the danger of ticks. In his book, “Forty Million Hoof Beats,” Heath recalled how he set off in 1925 to ride to all 48 American states. After more than 10,000 miles on the road he unknowingly rode into what was known as “an outlaw parish” in Louisiana. The entire county was so severely infested with disease-bearing ticks that the US government imposed a strict quarantine making it illegal for local residents to travel with their horses or take their animals off local farms. Having travelled so far, Heath pleaded with the government to allow him to complete the historic journey. He was eventually permitted to leave on the condition that he agreed to subject his mare, Gypsy Queen, to a severe anti-tick bath at a government facility. There she was immersed in a powerful liquid, then placed under strict quarantine for a week. After a careful full-body inspection, Gypsy Queen was given a tick-free certificate by a federal inspector, then immediately transported inside a sealed train car across the Mississippi River into tick-free territory. This image shows Frank and Gypsy Queen outside the White House in Washington DC on the concluding day of their 11,000 mile journey. |
 |
So, what happened to the Lyme vaccine?
Called LYMERix, it was approved and licensed in the U.S. in 1998. People were vaccinated. It was considered effective. But the timing was wrong. It came out at a time when vaccinations in general were under attack. Adverse reactions were reported. Anti-Lyme vaccine groups formed and a class-action lawsuit was filed. Sales were low. The vaccine was unprofitable. By 2002, it was withdrawn from the market. A similar vaccine under development in Europe was also dropped, so currently there is no vaccine available for humans though several are approved for dogs.
Now that Lyme is occurring in epidemic proportions, might a vaccine be coming soon?
A vaccine is still years away, a recent New York Times editorial concludes, though research is well under way and there is little doubt that it can be made. But it may well be blocked by a medical community which has yet to recognize that chronic Lyme disease even exists. Public opinion could make a difference, however.
There are now so many sufferers of Lyme that active organizations have been formed to increase awareness and raise funding for further research, improved testing, and speedier development of a safe vaccine. The International Lyme and Associated Diseases Society (ILADS) is an organization created by doctors for doctors willing to help patients with Lyme. They provide a very different set of guidelines for treating a tick-bite than the Infectious Diseases Society of America (IDSA). If there is a tick-bite, any kind of tick, and if there is redness and inflammation around the site beyond what is normal from a small scratch, tick-borne disease should be considered a possibility and treated accordingly.
There are numerous organizations which provide advocacy for patients seeking treatment for Lyme symptoms as well as research-based information to counteract the conservative IDSA position. In response, another conservative organization claims that their website is the only one which provides accurate information. Anyone researching Lyme or tick-borne disease needs to understand the controversies and the differences in information they or their doctors will encounter.
This is the politics of Lyme disease which makes treatment difficult. If caught early, a simple course of antibiotics is very likely to be effective.
Prevention is crucial, but not easy.
DEET, at 20 % concentration, is considered the “gold standard” in repellent sprays for humans, highly effective against ticks. Repellents with the ingredient picaridin, at 20% concentration, is thought to be a safer equivalent, approved in the U.S. in 2005 but used widely in Europe since the 1980’s. Another alternative is to spray or soak clothing, hats, boots and camping gear with permethrin, an effective insecticide which kills ticks on contact.
|
|
British Long Rider Mefo Phillips believes a tick latched onto her hair while she was bending down close to the grass to pound in a picket pin. This simple oversight resulted in a medical emergency. Long Riders can decrease the risk of exposure by wearing proper footwear and clothing while travelling in tick country. Wear a hat to protect your head. Wear long socks, long trousers and long-sleeved shirts. Keep your trousers tucked into your boots and your shirt sleeves buttoned tight at the cuff. If the tick infestation is especially bad, run tape around the top of your boots and the leg of your trousers so as to reduce their chance of entry. The key to turning your clothes into insect-repelling armour is by spraying them with a chemical known as permethrin. After you’re in the saddle and on the move, try to avoid brushing alongside tree branches. If you’re walking, stay in the centre of the trail, away from grass, so as reduce the chances of ticks attaching themselves to your legs |
Frequent body scans are crucial, looking for ticks or evidence of tick bites.
That’s how I found three imbedded ticks last spring when I was working and
recreating outdoors in Virginia. Recovering from Lyme, unfortunately, does not
provide immunity towards another infection. Sure enough, follow-up testing
indicated that I had an acute infection for Lyme, in other words, a recent
infection. So once again, I have undergone a more simplified treatment, though I
had no overt symptoms.
This is the dilemma of tick-borne disease. Do I trust the tests? Am I really free of symptoms? What about the joint pain that has escalated over the past year? Is it common arthritis that I had on a milder scale prior, or is it an exacerbation by Lyme pathogens hiding in my joints?
Anyone who lives or travels in the same area where ticks thrive can never be certain that he or she is free of tick-borne disease. A person can carry it without manifesting it until years later.
 |
Despite the march of time, some things never change for Long Riders. Being attacked by ticks is one such example. In the summer of 2012 Orion Kraus began his journey from Mexico to Panama. What did Orion finding waiting for him? “Ticks are the worst. My first night on the trail, I must have picked at least 20 ticks off me and I’ve been battling them ever since.” |
To compound a Long Rider’s concerns, there is the horse to consider.
Horses do get Lyme and other tick-borne diseases just as humans do and they can be tested just as humans are. Horse Journal reports that in endemic tick areas, as many as 75% of horses will test positive for antibodies to the Lyme pathogens. Not all will show symptoms or the symptoms may not present until months or years later. But for some horses, change in behavior or a new irritability may be the only sign that something is amiss. Intermittent lameness or shifting lameness from one leg to another may be another. Testing and treatment is expensive and chronic cases might include IV therapy which must be done at a clinic. And then, like people, horses can easily become re-infected.

|
The best prevention against your horse catching Lyme Disease is thoroughly grooming your horse every day to assure that any embedded ticks are caught and removed early. For example, during her journey from California to Maine Long Rider Sea G. Rhydr found this tick trying to attack her horse, Jesse James. Ticks hide deep in the animal’s hair, making them difficult to locate. They may be found by running your fingers slowly along the horse’s skin. When you locate a bump on the horse, avoid handling the tick with your uncovered fingers. Humans who pull off engorged ticks are in danger if they crush the vermin and are splashed with infected blood. Therefore care must taken. Wear rubber gloves and use a tick removal tool or a pair of tweezers to remove the pest. |
At the farm where I was working in the heart of Virginia horse country, ticks were commonly found on the horses, particularly those that were pastured. It is simply impossible to protect them all. The good news is that vaccinations are effective for dogs, and while they are not officially approved for equine use, it is becoming an increasingly common practice in endemic areas to use the dog vaccines for horses. Politics are not such an obstacle with animals. Moreover, Cornell University has developed an inexpensive and more sensitive test approved for horses called the Lyme Multiplex Assay which can differentiate between an acute and a chronic Lyme infection and also determine if a horse has already been previously vaccinated. In addition, it is effective 3-5 weeks after infection versus 6-8 weeks in the older tests.
Since the test provides a quantitative titer measurement for the number of antibodies present, it can be used to help evaluate the effectiveness of treatment as well. Pre-purchase exams in endemic areas are now including this test for a number of uses, including a simple baseline from which to detect change. A horse must also be disease-free prior to vaccination and often a month-long course of oral antibiotics is enough. So while our horses are more exposed to the bite of a tick than we are, detection through better tests and prevention through vaccines are more available for them. The Lyme Multiplex Assay is not approved for humans. A concern in the medical field is over-diagnosis of Lyme disease with tests of increased sensitivity.
Permethrin, the very effective insecticide which is not to be used on human skin except by prescription for treatment of scabies or head lice, is approved for direct use on horses as a spray or spot-on type of application. And as for humans, direct body checks for ticks are recommended, searching under the mane, in the throat latch, in the tender groin region, and under the tail in particular. Use of thin-tipped tweezers or a commercial tool is always recommended for tick removal versus pulling ticks off with the fingernails.
|
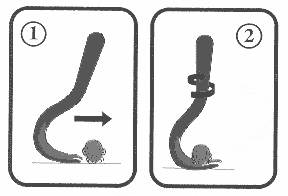
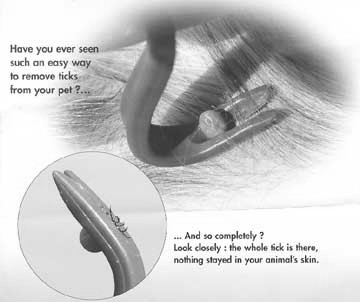
Should a tick manage to enter your clothes, it will often wander along your body for some time before deciding where to feed. By removing a tick without delay, you greatly reduce the chances of an infection being injected into your bloodstream. Therefore time is of the essence. At the conclusion of the day, a Long Rider must make an intensive body search for ticks. In truly bad tick country, plan to halt every two hours to search for ticks. First, inspect your clothes with great care. Wearing light-coloured clothes will help you detect the dark-coloured pests. Be especially attentive to the seams where ticks tend to hide. Next, inspect your body thoroughly. Ticks delight in concealing themselves in the warm, moist pubic area and armpits. Removing ticks from your own body requires care. The first thing to do is set aside the risky folk remedies which will increase the danger level. These tend to actually increase the risks of infection. The most popular and misguided method calls for smearing the tick with alcohol or petroleum. Another popular method is to touch the tick with a hot match head or to pass a lighted cigarette over it. People mistakenly believe that by covering the tick with a distasteful liquid, or exposing it to heat, it will voluntarily retract its head from within the victim’s body. What isn’t commonly known is that before doing so, the tick often regurgitates the poisonous contents of its stomach into the victim’s bloodstream. Thus, the folk remedies greatly increase the chances of infection. The best way to remove the pest is by using a small, plastic tick-removal tool. It has a two-pronged fork that slides between the skin and the tick. It can be carried in a shirt pocket so as to allow for quick access and has an excellent record of extractions. Tick removal tools are inexpensive and can be purchased in pet shops or in camping stores. |
The effects of Lyme disease go beyond pain and debilitation. Lyme is known to cause heart palpitations and to slow the heart rate to dangerous low levels. But Lyme hasn’t been considered a direct killer. A recent article in the Boston Globe, however, may prove otherwise.
Three abrupt deaths have occurred in the Northeast in the past 13 months which have been linked to inflammation of the heart related to Lyme disease. It was a doctor from a tissue bank who discovered an odd pattern in the heart of a man found dead in a car accident. The man was an organ donor. Testing showed that the man had unrecognized Lyme disease. The doctor had seen this heart pattern before in biopsies from people with Lyme disease. Fortunately, the heart was not implanted. Eight months later, the same doctor saw the same pattern in the heart of another donor who had collapsed at home. Tests came back for another case of Lyme. The CDC then got involved and began examining unexplained deaths to find yet another person who had collapsed and died, later to be found positive with the Lyme bacteria. None of the victims knew they had Lyme disease, but each had complained recently of symptoms indicative of Lyme. The victims were between the ages of 26 and 38.
Lyme can kill in another way.
In England recently, a double suicide occurred. After twenty years of disability that left her in a wheelchair and dependent on the care of her husband for most of her needs, a 44 year-old victim of Lyme disease took lethal medication obtained from Mexico. The husband was then arrested on suspicion of assisting in her suicide. While on bail, he too, ended his life.
It is beyond the scope of this article to cover every aspect of tick-borne disease that a Long Rider must consider. Nor is it meant to discourage a person from setting out to experience the natural world in the company of a horse.
What must be remembered is that knowledge is essential as is prevention and early treatment for a tick bite with any symptoms.
| After Long Rider Lucy Leaf completed her journey through the United States in the 1970s, she travelled 2,000 miles by dog team on two separate trips in Labrador. Because of her keen interest in medicine, Lucy has degrees in animal science and nursing. She is seen riding one of the Akhal Tekes which she trains in Virginia. |
|
For additional information on Lyme Disease:
http://www.ilads.org/lyme_disease/about_lyme.html
http://www.theguardian.com/environment/2013/sep/02/climate-change-crop-pests
http://www.wbur.org/2012/06/27/lyme-vaccine
http://www.horsenation.com/2013/05/22/eventing-nation-lyme-disease-knowlege-is-the-best-prevention/
http://emergency.cdc.gov/HAN/han00349.asp
Main Stories from the Road page